Infections make up more than 15% of presentations to emergency departments,1 but the broad range of presentations among patients with suspected infection can make precise diagnosis difficult.
Failing to identify and treat infection in a timely manner can lead to the development of severe infection and sepsis. However, the current lack of fast, accurate, and reliable testing options makes it difficult for providers to choose the correct course of action.
Patients presenting with similar symptoms can go down different paths. Some will improve and some deteriorate. Today’s tools are insufficient to help physicians make optimal clinical decisions.
With better tools to identify the source and severity of infection, providers can more confidently navigate the “gray zone” of patient presentations, with the insights to discharge patients who aren’t at risk and prioritize care for those who are at risk.
For example, patients with conditions such as severe pneumonia may be admitted to the ED and given antibiotics per hospital guidelines despite having a non-bacterial source of infection.2 Conversely, many patients at high risk for sepsis can appear well enough initially that diagnosis and treatment are delayed.3
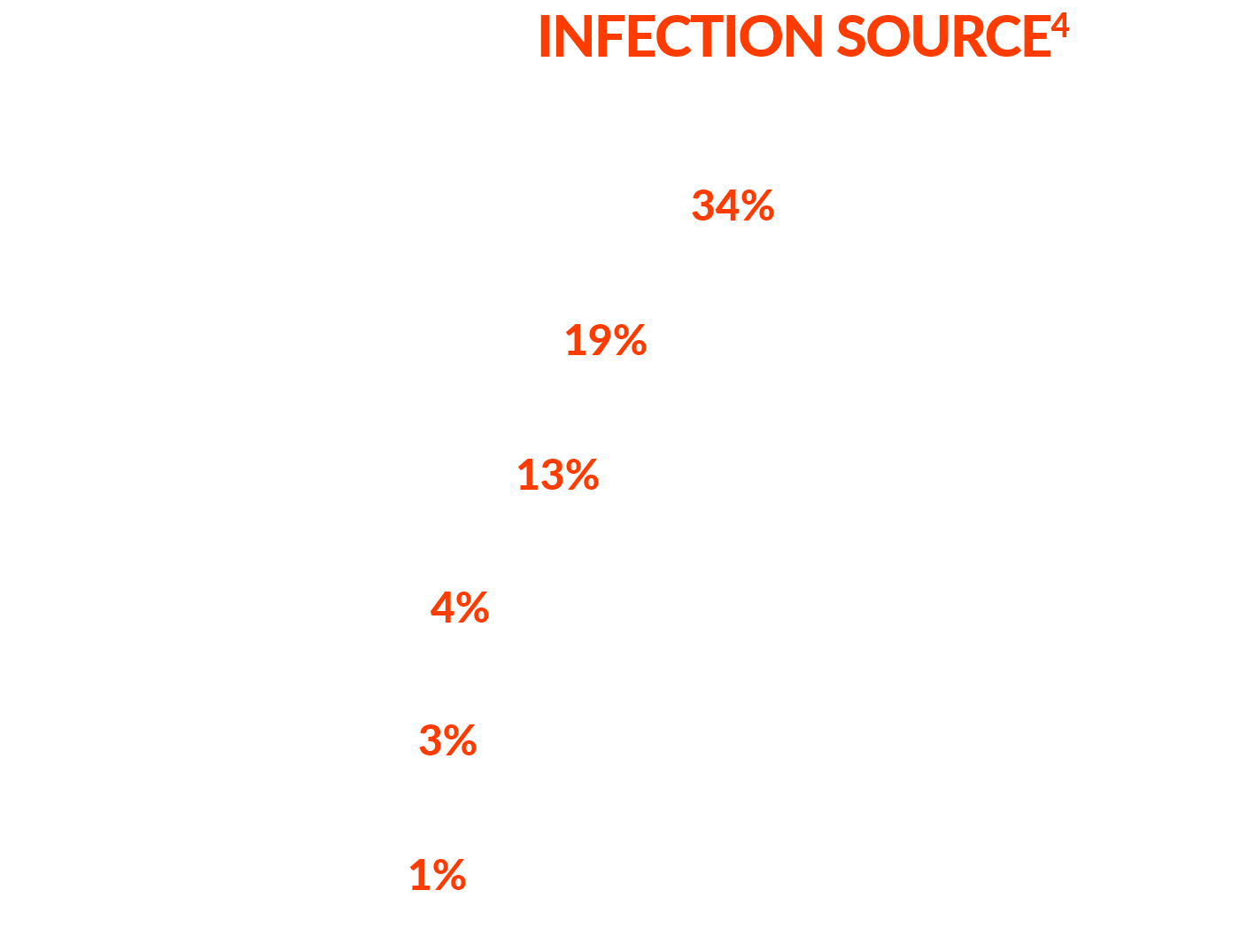
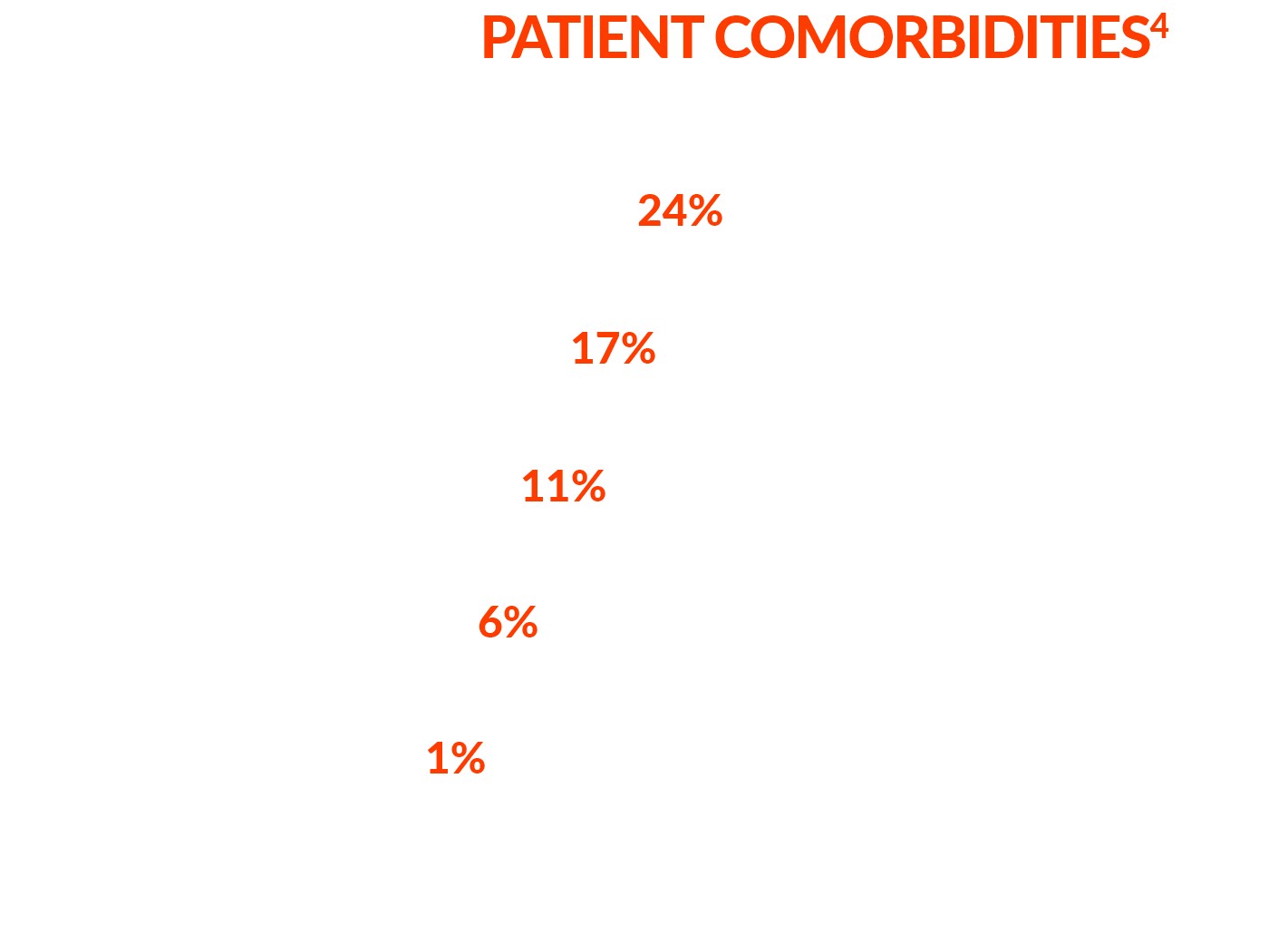
In one US study, patients evaluated in the ED for infection/sepsis were found to present with a wide variety of symptoms and comorbidities, making it hard to discern which individuals were most likely at risk of developing sepsis.4
While there are a variety of tests that may be used to screen for infection and sepsis, most of today’s tools are not equipped to provide FAST, ACTIONABLE, and RELIABLE results.
While commonly used to diagnose bacterial infections, blood cultures can be unreliable.
Most patients with confirmed infection based on clinical adjudication do not have positive microbiology to support the conclusion.
of patients with radiologically confirmed pneumonia did not have a causative pathogen IDENTIFIED BY COMPREHENSIVE MOLECULAR AND TRADITIONAL TESTING9
Early warning scores (EWS) such as the Systemic Inflammatory Response Syndrome (SIRS), Quick Sepsis-Related Organ Failure Assessment (qSOFA), National Early Warning Score (NEWS), Modified Early Warning Score (MEWS), or AI-assisted EHR tools, such as the Epic Sepsis Model, promote early diagnosis and provide standardization, but are prone to false positives in screening for sepsis,10,11 which may result in overdiagnosis, alert fatigue, and low adoption. For this reason, EWS may be recommended as screening tools for sepsis but are not wholeheartedly endorsed.12
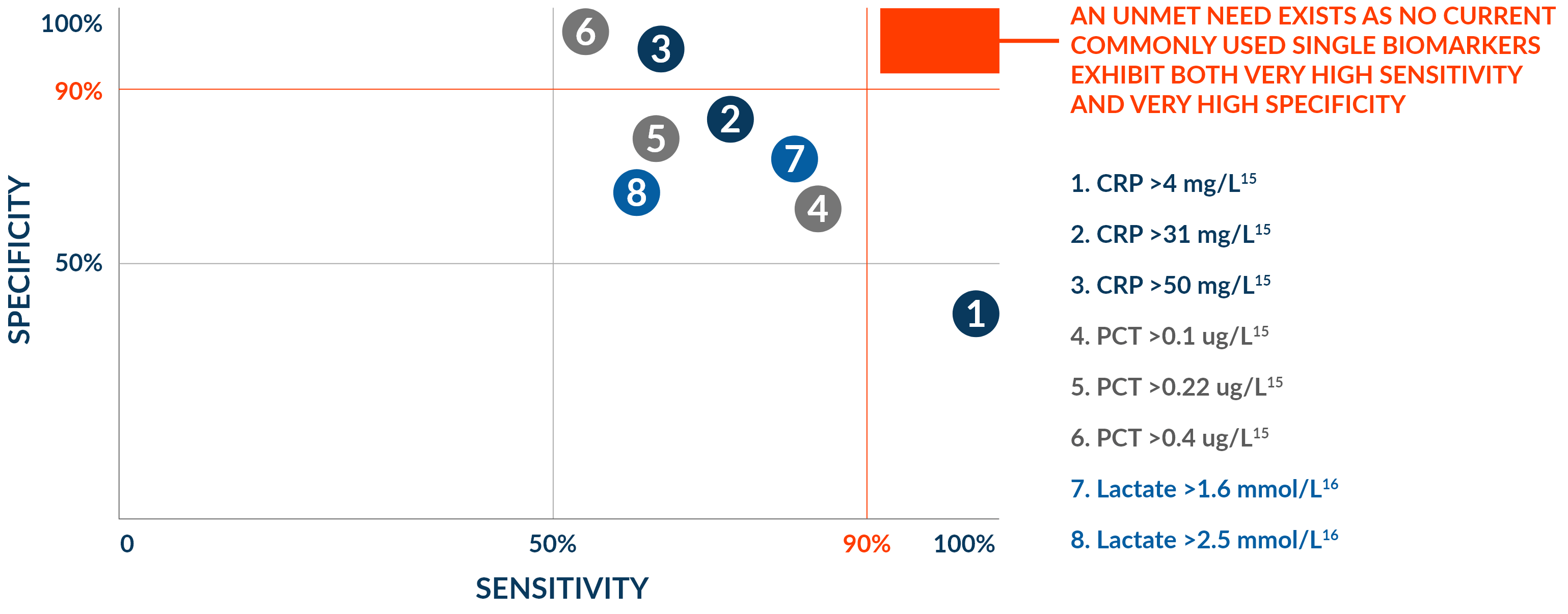
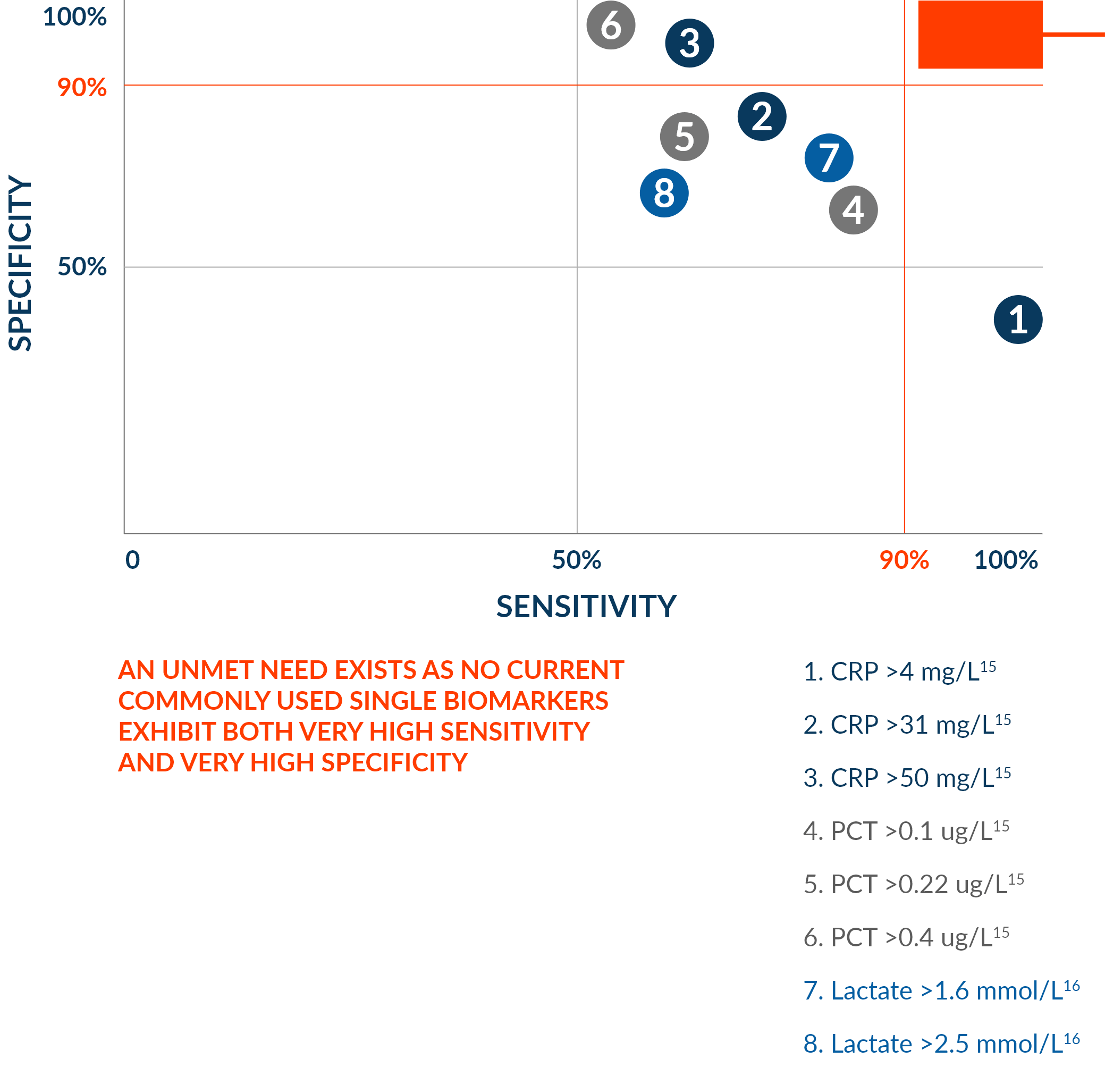
Testing for procalcitonin (PCT), C-reactive protein (CRP), lactate, and other biomarkers can be helpful in determining whether or not inflammation is present, but are neither sensitive nor specific enough for diagnosis when used alone.
Time pressures force quick decisions with limited information and negative consequences. At present, clinicians often lack tools to aid in their decision-making that combine both high accuracy and actionable results in a clinically relevant time frame.
This lack of available technology often leads to early treatment decisions, such as the decision to prescribe antibiotics, made empirically rather than based on a firm diagnosis. As a result, inappropriate antibiotics are prescribed as often as half of the time, leading to increased rates of drug-resistant organisms, opportunistic infections, and overall cost.17
Over the course of a 2-week hospital study, 30% of antibiotic prescriptions for non-critical hospitalized adult patients were found to be unnecessary.18
In another study, about 20% of patients given antibiotics in the hospital had a clinically significant antibiotic-associated adverse drug event within 30 days of antibiotic initiation.21
24% of bacterial isolates were multidrug resistant.20
Recent guidance still recommends treating the sickest patients immediately, within one hour of presentation.22
But for less sick patients, it suggests postponing the initiation of antibiotics until further assessments can be made, and more objective data become available to back clinical acumen.22
Identifying and evaluating an infection’s status and severity can provide a clearer idea of possible diagnostic and prognostic outcomes and allows care teams to make the most informed treatment decisions.
Additionally, by tailoring the level of care to the patient’s severity of infection, hospitals can reduce admissions and length of stay for less serious cases.

72-year-old female presents to the ED with abdominal pain in the LLQ, constipation, and anuria

Hypertension, urgent urinary incontinence

Pulse: 100
Blood pressure: 126/75
Respiration rate: 18
Temperature: 36.7 C
White blood cell count: 24 k
Lactate: 3.9 mol/L
Serum creatinine: 2 mg/dL
Urinalysis: Normal
Blood cultures: Pending
CT: Large stool volume in the descending and sigmoid colon without evidence of GI wall edema or hypoenhancement
Revealing the underlying cause in patients who present with similar symptoms can lead to better diagnostic decisions and treatment choices—resulting in better care and lower costs.
Better prescribing decisions and reduced morbidity and mortality from sepsis
Greater confidence in results and reduction in unnecessary further testing

Better level-of-care decisions informed by faster test results
Applicability across broader populations, demographics, and comorbidities
Learn more about how host response is redefining acute infection diagnosis and sepsis care